Stereotactic Radiosurgery (SRS) and Stereotactic Body Radiotherapy (SBRT)
What is stereotactic radiosurgery and how is it used? What equipment is used? Who will be involved in this procedure and who operates the equipment? How is the procedure performed? Is there any special preparation needed for the procedure? What will I feel during and after this procedure?Overview
Stereotactic radiosurgery (SRS) is a non-surgical radiation therapy used to treat functional abnormalities and small tumors of the brain. It can deliver precisely-targeted radiation in fewer high-dose treatments than traditional therapy, which can help preserve healthy tissue. When SRS is used to treat body tumors, it's called stereotactic body radiotherapy (SBRT).
SRS and SBRT are usually performed on an outpatient basis. Ask your doctor if you should plan to have someone drive you home afterward and whether you should refrain from eating or drinking or taking medication several hours before treatment. Tell your doctor if there's a possibility you are pregnant or if you're breastfeeding or if you're taking oral medication or insulin to control diabetes. Discuss whether you have an implanted medical device, claustrophobia or allergies to contrast materials.
What is stereotactic radiosurgery and how is it used?
Stereotactic radiosurgery (SRS) is a highly precise form of radiation therapy initially developed to treat small brain tumors and functional abnormalities of the brain. The principles of cranial SRS, namely high precision radiation where delivery is accurate to within one to two millimeters, are now being applied to the treatment of body tumors with a procedure known as stereotactic body radiotherapy (SBRT).
Despite its name, SRS is a non-surgical procedure that delivers precisely-targeted radiation at much higher doses, in only a single or few treatments, as compared to traditional radiation therapy. This treatment is only possible due to the development of highly advanced radiation technologies that permit maximum dose delivery within the target while minimizing dose to the surrounding healthy tissue. The goal is to deliver doses that will destroy the tumor and achieve permanent local control.
SRS and SBRT rely on several technologies:
- three-dimensional imaging and localization techniques that determine the exact coordinates of the target within the body
- systems to immobilize and carefully position the patient and maintain the patient position during therapy
- highly focused gamma-ray or x-ray beams that converge on a tumor or abnormality
- image-guided radiation therapy (IGRT) which uses medical imaging to confirm the location of a tumor immediately before, and in some cases, during the delivery of radiation. IGRT improves the precision and accuracy of the treatment
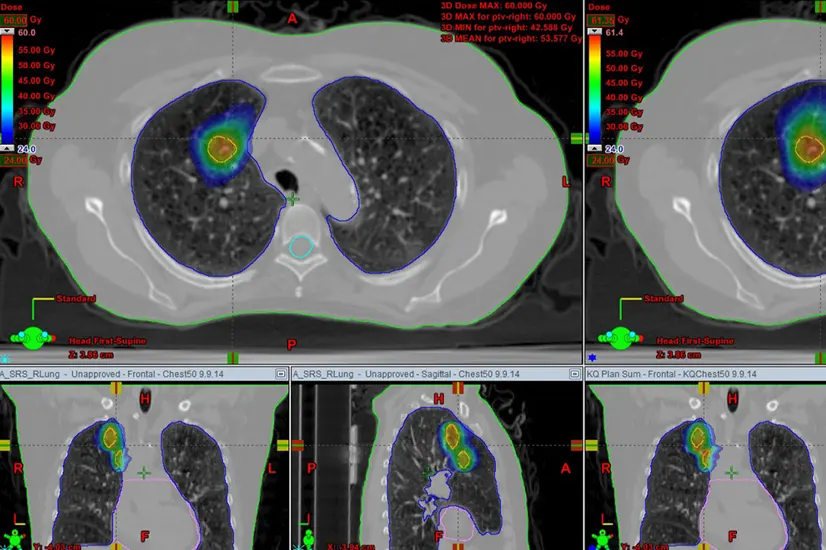
Three-dimensional imaging, such as CT, MRI, and PET/CT is used to locate the tumor or abnormality within the body and define its exact size and shape. These images also guide the treatment planning—in which beams of radiation are designed to converge on the target area from different angles and planes—as well as the careful positioning of the patient for therapy sessions.
Although SRS commonly refers to a one-day treatment, physicians sometimes recommend multiple stereotactic delivered treatments. This is important for tumors larger than one inch in diameter as the surrounding normal tissue exposed to the single high dose of radiation must be respected and limited, and the volume of normal tissue treated increases proportionally to the tumor size. Delivering the radiation in a few sessions as opposed to one, can improve safety and allow the normal tissue to heal in between treatments. Therefore, fractionating the treatment allows for high doses to still be delivered within the target, while maintaining an acceptable safety profile. This procedure is usually referred to as fractionated stereotactic radiotherapy (SRT), and typically refers to the delivery of two to five treatments of focused radiation and are not always given on consecutive days.
SRS and SBRT are important alternatives to invasive surgery, especially for patients who are unable to undergo surgery and for tumors and abnormalities that are:
- hard to reach
- located close to vital organs/anatomic regions
- subject to movement within the body
SRS is used to treat:
- many types of brain tumors including: benign and malignant, primary and metastatic, single and multiple, residual tumor cells following surgery, intracranial, orbital and base-of-skull tumors
- arteriovenous malformations (AVMs), a tangle of expanded blood vessels that disrupts normal blood flow in the brain and sometimes bleeds.
- other neurological conditions like trigeminal neuralgia (a nerve disorder in the face), tremor, etc.
SBRT is currently used and/or being investigated for use in treating malignant or benign small-to-medium size tumors in the body and common disease sites, including the:
- lung
- liver
- abdomen
- spine
- prostate
- head and neck
SRS fundamentally works in the same way as other forms of radiation treatment. It does not actually remove the tumor; rather, it damages the DNA of tumor cells. As a result, these cells lose their ability to reproduce. Following treatment, benign tumors usually shrink over a period of 18 months to two years. Malignant and metastatic tumors may shrink more rapidly, even within a couple of months. When treated with SRS, arteriovenous malformations (AVMs) may begin to thicken and close off slowly over a period of several years following treatment. Many tumors will remain stable and inactive without any change. Since the aim is to prevent tumor growth, this is considered a success. In some tumors, like acoustic neuromas, a temporary enlargement may be observed following SRS due to an inflammatory response within the tumor tissue that overtime either stabilizes, or a subsequent tumor regression is observed called pseudoprogression.
What equipment is used?
There are three basic kinds of equipment, each of which uses different instruments and sources of radiation. At GSRO, we utilize TrueBeam's linear accelerator:
- Linear accelerator (LINAC) machines, prevalent throughout the world, deliver high-energy x-rays, also known as photons. The linear accelerator can perform SRS on larger tumors in a single session or during multiple sessions, which is called fractionated stereotactic radiotherapy. Multiple manufacturers make this type of machine, which have brand names such as TrueBeam™, Novalis Tx™, XKnife™, Axesse™ and CyberKnife®.
- The Gamma Knife®, which uses 192 or 201 beams of highly focused gamma rays all aiming at the target region. The Gamma Knife is ideal for treating small to medium size intracranial lesions.
- Proton beam or heavy-charged-particle radiosurgery is in limited use in North America, though the number of centers offering proton therapy has increased dramatically in the last several years.
Who will be involved in this procedure and who operates the equipment?
The treatment team is comprised of a number of specialized medical professionals, typically including a radiation oncologist, medical radiation physicist, radiologist, dosimetrist, radiation therapist, and radiation therapy nurse.
- The radiation oncologist and, in some cases, a neurosurgeon lead the treatment team and oversee the treatment; they outline the target(s) to be treated, identify any sensitive tissues or organs at risk, decide on the appropriate radiation dose, approve the treatment plan, and interpret the results of radiosurgical procedures.
- A radiologist interprets imaging that identifies the target(s) to be treated in the brain or body.
- The medical radiation physicist ensures the delivery of the precise dose of radiation.
- The physicist, or a dosimetrist under the supervision of the physicist, uses special computer software to devise a treatment plan; he or she calculates the exposures and beam configuration to conformally treat the target(s) to the prescribed dose.
- A highly trained radiation therapist positions the patient on the treatment table and operates the machine from an adjacent protected area. The radiation therapist can observe the patient through a window or on a closed-circuit television and is able to communicate with the patient throughout the procedure.
- The radiation therapy nurse assesses the patient, provides the patient with information about the treatment, monitors the patient during treatment, and helps answer questions after treatment.
- A neurologist or neuro-oncologist may participate with the radiation oncologist and neurosurgeon in the multidisciplinary team that considers various treatment options for individual cases and helps decide who may benefit from radiosurgery for lesions in the brain.
How is the procedure performed?
Radiosurgery Using the Linear Accelerator:
Linear accelerator (LINAC) SRS is similar to the Gamma Knife procedure and its four phases: head frame placement, imaging, computerized dose planning and radiation delivery. LINAC technology is much more common than Gamma Knife technology and has been in practice for a similar length of time. Unlike the Gamma Knife, which remains motionless during the procedure, part of the LINAC machine (called a gantry) rotates around the patient delivering the radiation beams from different angles. Obtaining the MRI before frame placement is also a more routine pre-planning practice with LINAC-based SRS. A CT with the frame in place is also commonly acquired.
SBRT:
SBRT typically consists of one to five treatment sessions delivered over the course of one to two weeks.
For some technologies like the CyberKnife that base image-guidance according to an x-ray based solution, you may be asked to have a fiducial marker placed in or near your tumor for selected cases. However, for most CT based image-guidance technologies, this step is not needed. If a fiducial is required, depending on the location of your tumor, your radiation oncologist may work with a pulmonologist, gastroenterologist or radiologist to have one to four fiducial markers placed near the tumor. Placement of the fiducial marker is almost always an outpatient procedure.
Next, your radiation oncologist will determine the method of aligning your body with the beams from the linear accelerator, which is called a simulation. Immobilization devices are often used to align patients very precisely and make sure they remain still during simulation and treatment. Some of these systems may hold you quite tight; therefore you should tell your physician if you suffer from claustrophobia. After an immobilization device is created for you, a CT scan is performed over the area to be treated. Your physicians may also perform a '4DCT,' where the CT scan obtains information on how your tumor moves while you breathe. This is very common for tumors in the lungs or liver. After the scan is completed, you will be sent home.
The third part of the course is planning. The radiation oncologist will work with a radiation dosimetrist and medical physicist to plan the beam arrangement best suited for your tumor. They may incorporate other imaging techniques, such as MRI or PET/CT. Using specialized software, the team will go through hundreds of different combinations of beams to figure out which would be best for your situation.
Radiation delivery of SBRT is done on a linear accelerator. There are normally no restrictions on eating or drinking, though some patients may take an anti-inflammatory, anti-nausea or anti-anxiety medication prior to the treatment. You will be placed in the immobilization device. X-rays or a CT scan (depending on the mode of image-guidance specific to the LINAC technology) will be taken to line up the beams of radiation with the tumor prior to starting the radiation therapy. The radiation therapist will position you with guidance from the radiation oncologist based on these x-rays. The radiation therapist will then deliver the treatment. Sometimes, x-rays or a CT scan will be taken during the treatment to monitor the position of the tumor. Treatment can take up to one hour or more.
Is there any special preparation needed for the procedure?
SRS and SBRT are usually performed on an outpatient basis. However, be prepared to spend up to a half-day or more at the facility. You will be informed whether you need to have someone accompany you and drive you home afterward.
You may be asked not to eat or drink anything after midnight on the night before your treatment. You should ask your physician about taking any medications on the day of your treatment and bring those medications with you to the procedure. You should also tell your physician if any of the following apply to you:
- You are taking medications by mouth or insulin to control diabetes.
- You are allergic to intravenous contrast material or iodine.
- You have a pacemaker, artificial heart valve, defibrillator, brain aneurysm clips, implanted pumps or chemotherapy ports, neurostimulators, eye or ear implants, stents, coils or filters.
- You suffer from claustrophobia.
What will I feel during and after this procedure?
Radiosurgery treatments are similar to having an x-ray. In general you will not be able to see, feel or hear the x-rays. One exception is that some patients who are having treatments to the brain may see flashes of light while the machine is on, even with their eyes closed. There is no pain or discomfort from the actual treatment.
If you experience pain for other reasons, such as back pain or discomfort from the head frame or immobilization device, you should let your doctor or nurse know.
When the head frame is removed, there may be some minor bleeding from the pin sites that will be bandaged. You may experience a headache and can ask for medication to help make you feel more comfortable.
In most cases, radiosurgery and SBRT patients can resume all of their normal activities within one or two days.
Side effects of radiation treatment include problems that occur as a result of the treatment itself as well as from radiation damage to healthy cells in the treatment area.
The number and severity of side effects you experience will depend on the type of radiation and dosage you receive and the part of your body being treated. You should talk to your doctor and nurse about any side effects you experience so they can help you manage them.
Radiation therapy can cause early side effects during or immediately after treatment, and are typically gone within a few weeks. Late side effects can occur months or years later. Common early side effects of radiation therapy include tiredness or fatigue and skin problems. Skin in the treatment area may become more sensitive, red, irritated, or swollen. Other skin changes include dryness, itching, peeling and blistering.
Depending on the area being treated, other early side effects may include:
- hair loss in the treatment area
- mouth problems and difficulty swallowing
- eating and digestion problems
- diarrhea
- nausea and vomiting
- headaches
- soreness and swelling in the treatment area
- urinary and bladder changes
Late side effects may occur months or years following treatment. While they are often permanent, they are rare. They include:
- brain changes
- spinal cord changes
- lung changes
- kidney changes
- colon and rectal changes
- infertility
- joint changes
- lymphedema
- mouth changes
- secondary cancer
There is a slight risk of developing cancer from radiation therapy. After treatment, your radiation oncologist will regularly check for complications and recurrent or new cancers.
Using techniques such as SBRT, the aim is to maximize the cancer-destroying capabilities of radiation treatment while minimizing its effect on healthy tissues to limit the side effects of the treatment itself.